Want to get a tan but not sure if today’s the right day? Before you go out in the sun, it’s a good idea to check something called the UV Index. That’s the number you see on weather apps; it
Are you curious about how many albums Drake has released so far? We have got you covered! From his start on Degrassi to becoming one of the biggest names in music, Drake has dropped hit after hit. But with studio
Ivan Cornejo is a young and famous singer in the Latin music industry. He is remembered as an emotional singer, with soft voice and contemporary regional Mexican style of music. There are numerous fans who go online to get to
Welcome to cuindependent, your space for bold ideas, fresh perspectives, and engaging stories. We bring you content that informs, inspires, and sparks conversation.
From inspiring artistry to achievements in sports and beyond, we bring the highlights. A curated view of stories shaping conversations across fields today.
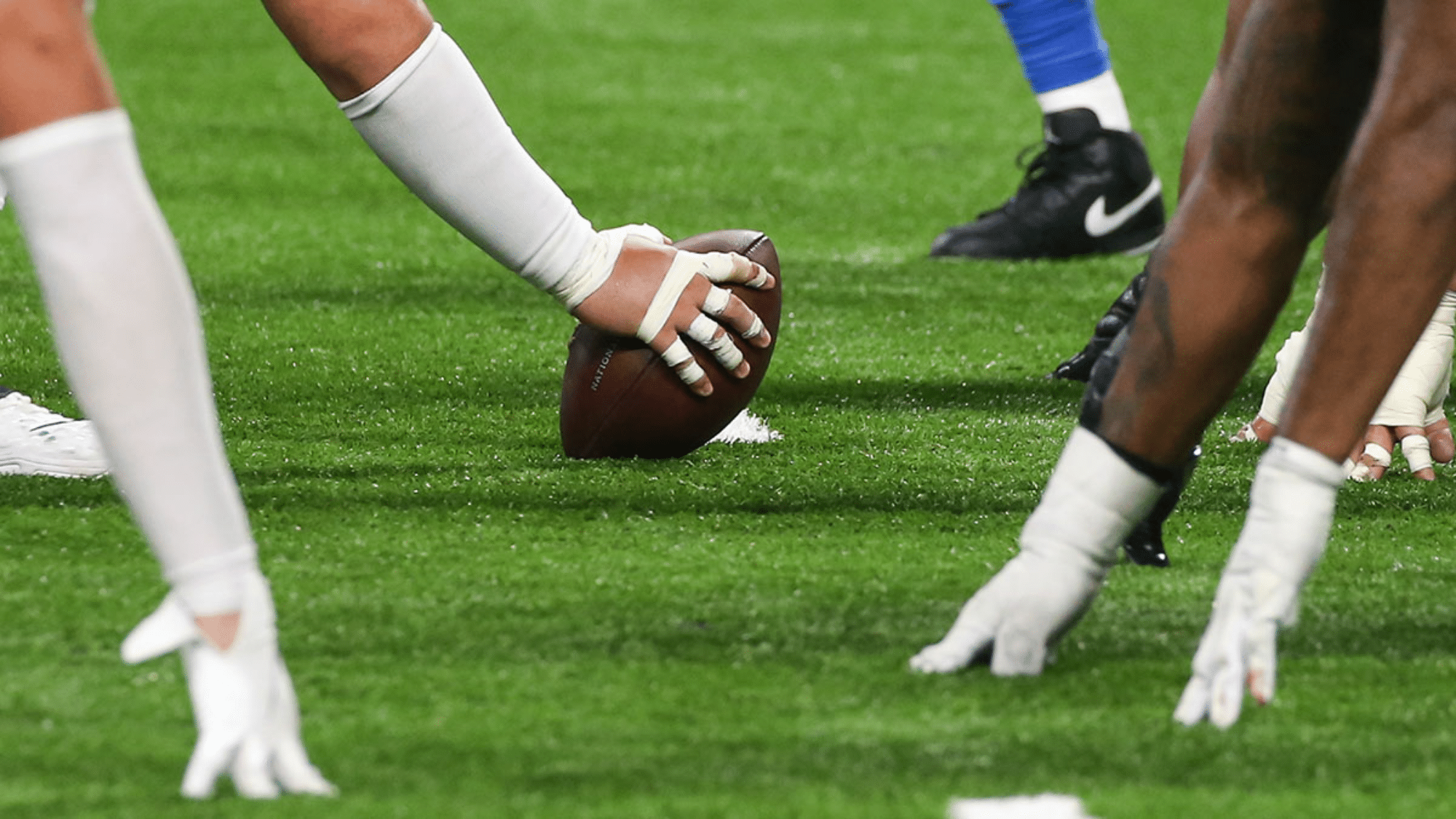
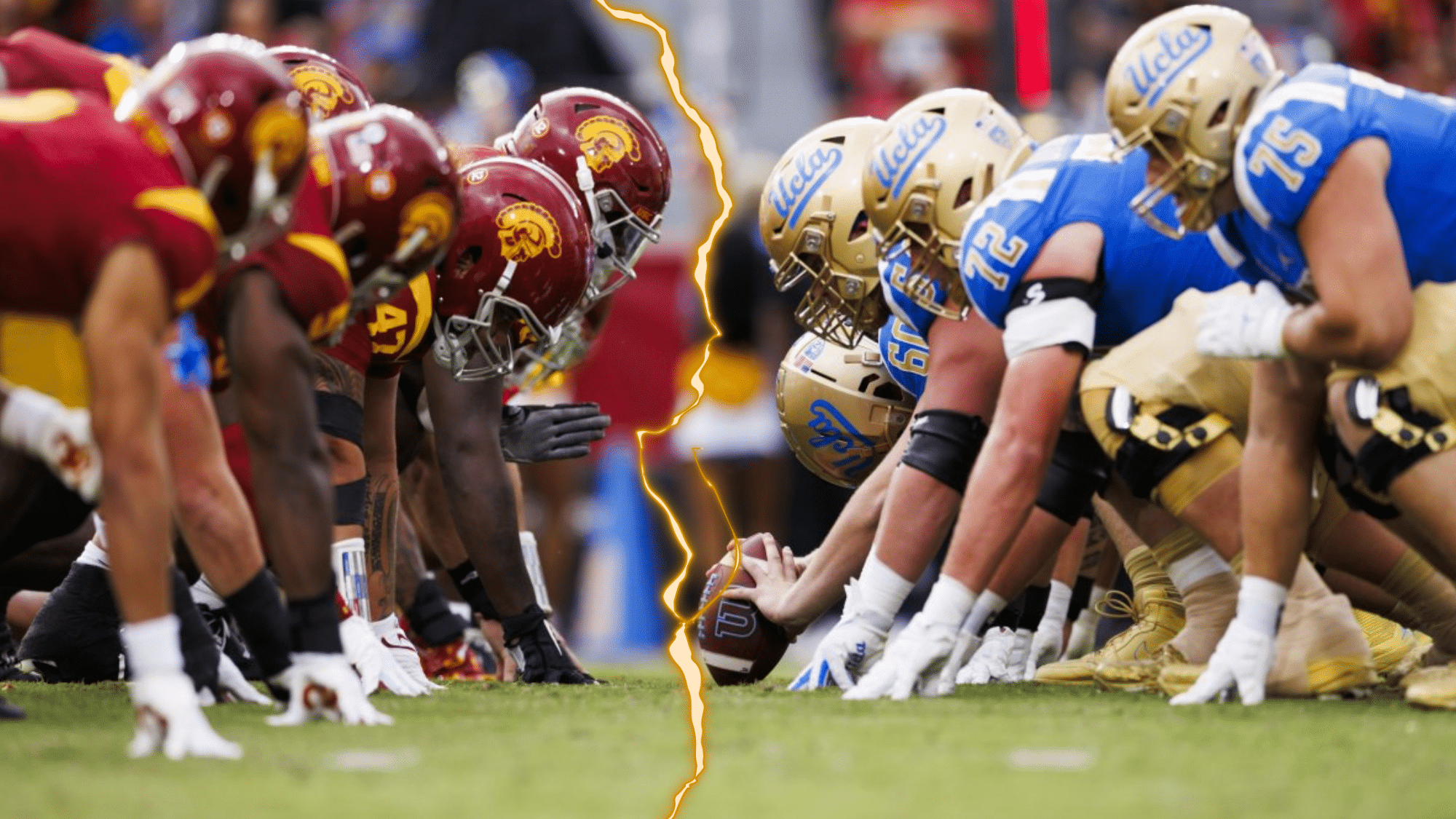
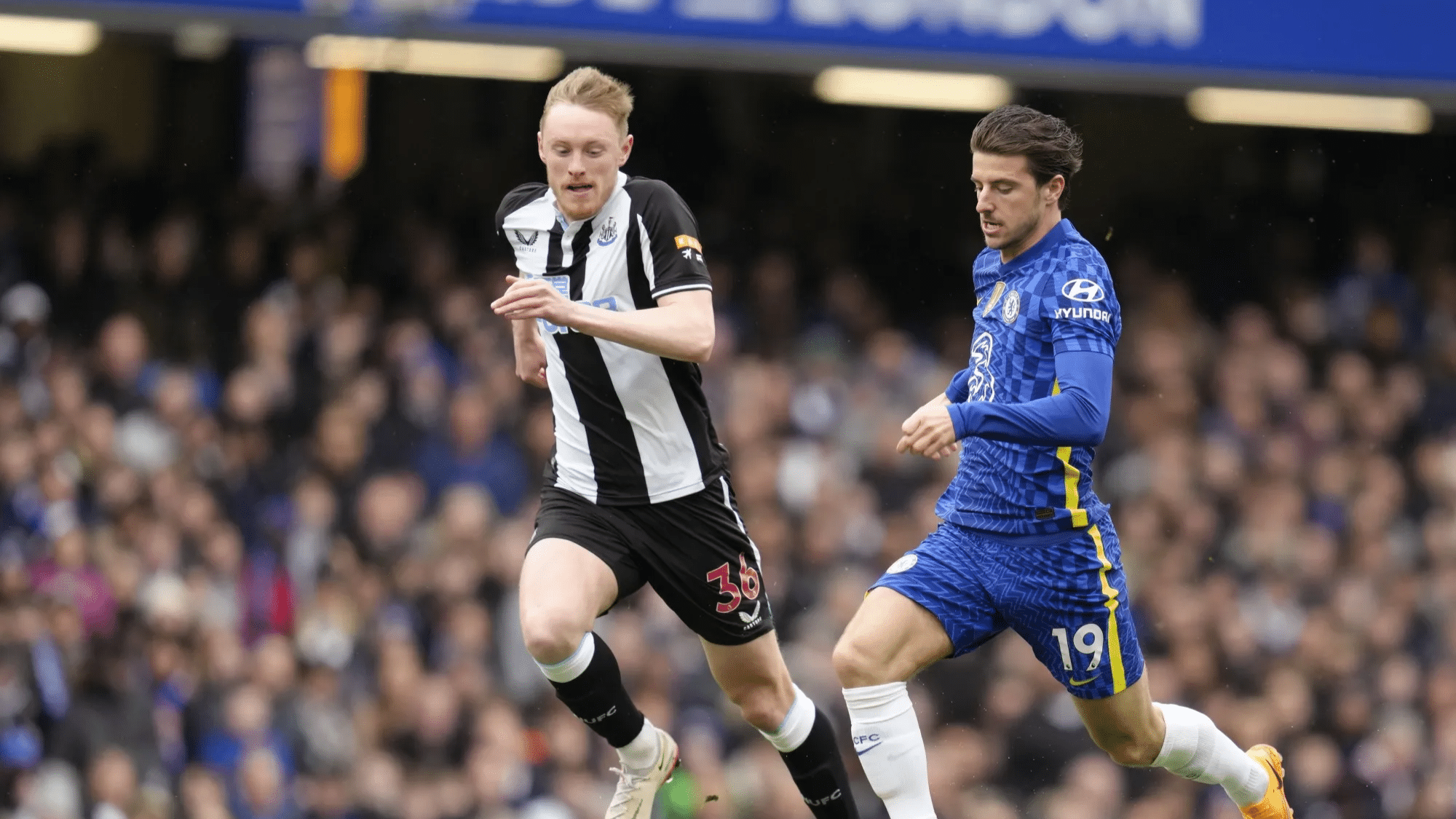
Some games aren’t just played, they are felt in the soul. These iconic rivalries go beyond the scoreboard, turning into battles of pride, passion, and identity that echo across generations. Whether it’s football in Argentina or cricket in India, these matchups light up stadiums, stir entire nations, and write unforgettable chapters.....
Walk into a room with a well-made piano and something shifts before a single key is pressed. There is a presence to a serious instrument that a purely functional one never quite achieves, and anyone who has spent time around both learns to feel the difference almost instantly. That difference is.....
At CU Independent, we’re committed to delivering real, bold, and honest stories. Get to know the passionate team behind the content!
With 10+ years in journalism and specialization in current events and social issues, Samantha leads the team with a commitment to diverse, inclusive storytelling.
She ensures CU Independent remains a platform for honest conversations about identity, sexuality, and culture.
★★★★★Rated 5 out of 5
Samantha Lee
(Editor-in-Chief)
A Ph.D. in Sociology and certified sex educator, Alex pens in-depth articles on identity and societal norms, bringing a research-driven approach to complex issues like sexuality and intersectionality.
Hootie & the Blowfish is a beloved American rock band, best known for their chart-topping hits in the 1990s. Formed in 1986 in Charleston, South Carolina, the band quickly rose to fame with their unique blend of pop, rock, and blues. Their catchy songs and relatable lyrics connected with fans, making.....
Want to get a tan but not sure if today’s the right day? Before you go out in the sun, it’s a good idea to check something called the UV Index. That’s the number you see on weather apps; it tells you how strong the sun’s rays are and how likely.....
Denim has a way of refusing to stay in its lane. What started as workwear became a canvas for every subculture imaginable, and right now the loudest denim story going is the return of jorts. Those cut-off, knee-grazing shorts your favorite indie band probably wore in a grainy music video are.....
The nomadic lifestyle isn’t for everyone. But it might be for you. Most people spend years in the same city, with the same routine, the same four walls. And for a lot of them, that works just fine. But some people hit a point where something feels off. Not broken, just.....
Taylor brings eight years of experience covering the indie music scene, exploring how music connects with culture and self-expression.
Maya, with a sociology background, writes about relationships, mental health, and navigating identity with an empathetic approach.Her passion for helping people create better habits and live more fulfilling lives.
As a fashion editor by profession, Rachel also focuses on painting, sculpture, and modern artistic expressions, aiming to make the world of fine arts more approachable for everyone.
Chris, a dedicated LGBTQIA+ activist, shares both personal stories and advice on queer and transgender issues, offering empowering content for the community.
Elliot oversees social media and audience engagement, ensuring CU Independent connects meaningfully with readers and builds a supportive online community.